Hazards
-
Natural hazards come in many forms: volcanic activity, earthquakes,
and asteroid impacts are all examples of natural hazards. Harmful agents
present in the environment also constitute a natural hazard.
example: asteroid impacts
-
The Earth's Moon is heavily cratered as a result of asteroid impacts over
its history, and numerous craters have also been preserved in continental
regions of the Earth. Plate-tectonic activity has probably destroyed the
evidence of many other asteroid impacts. In 1908, a meteorite crashed into
the Earth (or, possibly, exploded just over the Earth's surface) in a
remote region of Siberia. The Tunguska meteorite, as it has come to be
known, did a great deal of damage, but because the area it landed in was
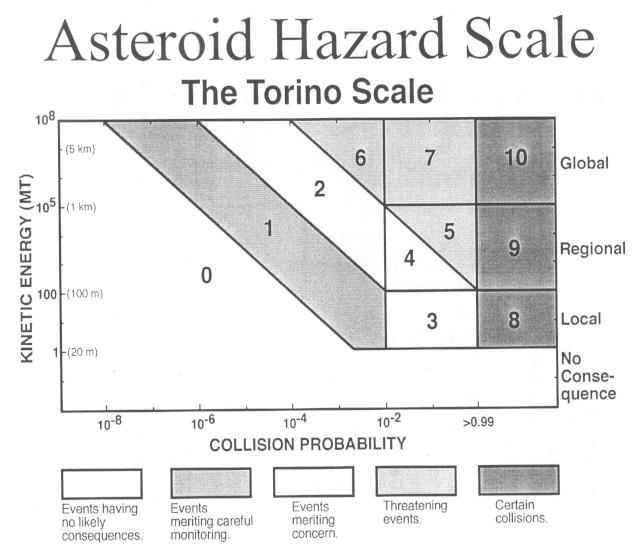
remote and unpopulated, no people were injured or killed. Asteroid impacts
are clearly a hazard; the Torino scale uses the kinetic energy of an
asteroid and the probability that it will collide with the Earth to assess
asteroid hazards. A small asteroid is of little hazard, whereas a large
asteroid with high kinetic energy could have catastrophic consequences
globally if it were to hit the Earth. How much of a risk to human life an
asteroid impact poses depends on variables such as the location of the
impact, in addition to the size and kinetic energy of the impacting object.
[ the Torino scale ]
Risks
-
The term "risk," as used in everyday parlance, is often synonymous
with "hazard." Here, however, we will use a more specific definition:
Risk is the probability that exposure to a hazard will lead to
negative consequences. The distinction is important for discussions
of mitigation of natural hazards.
example: Mt. Everest
-
To illustrate this distinction, and its importance, consider the hazards
and risks associated with climbing Mt. Everest. Mt. Everest is a hazardous
place, with severe weather and cold, and little oxygen in the air.
For those who attempt to climb Mt. Everest, the risk is high: in 1993,
129 climbers reached the summit, and eight died (a ratio of 16:1); in
1996, 98 climbers summitted, and 15 died (a ratio of 6:1). The risk
to the climbers -- here, the probability of death -- was high in both
years, though slightly lower in 1993. The risk to anyone who did not
attempt the climb, however, was zero. When an individual or group is
not exposed to a hazard, they face no risk from that hazard.
risk perception
-
How risks are perceived depends on a variety of factors in addition
to the actual risk due to a particular hazard. One of the most important
factors is the voluntariness of exposure to a hazard. In the example
above, exposure to the hazards associated with climbing Mt. Everest
was voluntary. Similarly, cigarette smoking is a voluntary activity
(excluding here issues related to secondhand smoke). Exposure to hazards
like asteroid impacts and harmful substances in the environment is
involuntary. Most people are willing to accept a higher level of risk when
exposure to a hazard is voluntary, as it is in the cases of mountain
climbing and cigarette smoking.
-
How commonplace or rare the consequences of a hazard are will also
influence risk perception. For example, personal acquaintance with
someone affected by a particular hazard may influence awareness of
the risk, and/or the sense that one is at risk oneself. Recognized
and unrecognized risks will also be perceived differently, as will
risks related to great disasters versus those associated with
minor or isolated incidents.
-
The emotional impact of a particular risk is also an important factor
for risk perception. For example, the terrorist attacks in
New York, Washington, and Pennsylvania in September of 2001, which
killed approximately 3,000 people, were very traumatic. In the same
month, approximately 3,000 people died in traffic accidents; approximately
the same number of people have died in traffic accidents in every
month since. While the lives lost in traffic accidents are no less
valuable than those lost in the terrorist attacks, the emotional
impact is substantially different.
-
All of the factors that affect risk perception are important in the
mitigation of natural hazards, since they have a strong impact on
public policy.
Respiratory diseases, asbestos, and radon
-
Asbestos and radon both pose a hazard to human health, since exposure
to either of these natural materials can, under certain circumstances,
lead to serious respiratory diseases, including cancer. The risks we
face from these hazards depend on a variety of factors, and, particularly
in the case of asbestos, the risks are poorly understood by policy
makers, and, consequently, by the public. It is worth noting that
smoking eclipses all other causes of respiratory disease. The risks
due to smoking are so large that they often interfere with attempts
to measure and understand the effects of other hazards.
occupational vs. non-occupational exposure
-
It is important to distinguish between occupational and non-occupational
exposure to hazards such as asbestos. Individuals who work routinely with
hazardous materials, or in a setting where exposure to hazardous materials
occurs regularly, are exposed to much higher concentrations of those
hazardous materials than is the general public. Occupational exposure to
asbestos occurs, for example, for asbestos miners and (formerly) people
employed to weave textiles including asbestos fibers. Most of the
information that we have linking specific diseases to exposure to harmful
materials comes from studies of those exposed to these hazardous materials
in occupational settings-- i.e., at very high concentrations.
-
It is often impossible to assess the impact of non-occupational (low-dose)
exposure directly, since many other factors intervene. As a result,
the risk related to non-occupational exposure is often determined (or
guessed at) by extrapolation of results based on occupational exposure.
Without a biological model for the relationship between exposure and
disease, however, it is hard to know what the best approach for
extrapolating from available data might be. The schematic graph below
shows three possible extrapolations from the same data set. The line
drawn on such a graph is referred to as a dose-response curve, or a
dose-response model.
asbestos
-
Lots of money has been, and continues to be, spent on mitigation of the
asbestos hazard. A chart showing the lifetime risk of premature death
from exposure to asbestos in school buildings compared with the risk from
various other hazards is attached. The risk due to asbestos is very
small in comparison with many other risks, such as those due to consuming
Miami or New Orleans drinking water, diagnostic x-rays, or smoking.
The small risk due to asbestos exposure, particularly in comparison
with these other, much larger, risks, suggests that our money might
be better spent elsewhere.
[ table with lifetime
risks of premature death ]
-
Many definitions of asbestos exist; the industrial definition of asbestos
states that it is a material having an aspect ratio (length to width)
of at least 3:1, with a fiber length of at least 5 microns. The definition
includes many different minerals, from two groups. Chrysotile, an asbestos
mineral of the serpentine group, is a sheet silicate that accounts
for about 95% of industrial asbestos production during the last 100 years.
It is the least hazardous of the asbestos minerals, especially in
non-occupational settings. The amphibole asbestos minerals have a crystal
structure in which silica tetrahedra are linked in double chains, as
with the other amphibole minerals we have discussed. The differences in
crystal structure and chemistry between the two groups of asbestos minerals
lead to differences in physical properties. Both can be fibrous, with
large aspect ratios, but chrysotile fibers tend to be flexible and
curled, a result of a space mismatch between layers in the sheet structure.
Crocidolite and the other amphibole asbestos minerals tend to be rigid
and needlelike owing to their double-chain structure. These differences
in physical properties have important implications for the potential of
the different minerals to damage the lungs.
[ asbestos minerals and
varieties ]
-
The respiratory system begins at the top with the wind pipe, which
then branches and rebranches multiple times in the lungs, forming
the bronchial tree. At the finest level of branching, each branch
ends in a small, grape-like sac where the gas exchange between air
and blood occurs; these sacs are known as pleura. The entire bronchial
tree is enclosed by the pleural sac. Anything that injures the pleura
or the pleural sac impairs gas exchange and the ability to breathe.
Respiratory disease can be caused by the inhalation of particulate matter
that gets stuck in the wall of the lung, particularly in the pleura.
-
One of the serious diseases associated with asbestos inhalation is
mesothelioma, a rare cancer of the lung. It appears to be caused
by the lodging of asbestos fibers in the pleura or the pleural sac.
Amphibole varieties of asbestos, most notably crocidolite, can
penetrate the pleura and the pleural sac as a result of their
needlelike shape and resistance to dissolution (and hence long residence
time) in lung fluids and tissue. Chrysotile asbestos, however,
will not generally be inhaled as deeply into the lungs, due to
its flexibility and curly shape. When it does enter the lungs, chrysotile
dissolves quickly, within a few weeks. It is thus very difficult
for chrysotile to have the negative effects on respiratory health
described for crocidolite.
-
Epidemiological studies -- studies that compare patterns of disease and
death with other patterns, such as exposure to a given substance -- show
that, in fact, there have been many extra deaths from crocidolite
exposure in occupational settings, particularly due to mesothelioma. This
is not true, however, for chrysotile. The relative risks, all from studies
of occupational exposure, are shown in the table attached. The risk from
exposure to chrysotile is quite low (the risk cited in the table of excess
mortalities above is a maximum estimate, since it was calculated without
taking into account the differences between chrysotile and the
amphibole asbestos minerals).
[ proportional mortality due
to occupational exposure to asbestos ]
-
Considering the important differences between the asbestos minerals,
and the facts that chrysotile is by far the most common asbestos mineral
present in buildings and that the risk from chrysotile exposure is
very low, the public policy decision to lump all asbestos minerals
together and to require their removal from public buildings is not
a good one. It is very difficult at this point to have a rational,
public debate about asbestos. The public fear factor is high, asbestos
exposure is an involuntary risk, and many vested interests (those
who profit from asbestos litigation and those who earn money removing
asbestos from buildings) are opposed to changes in current public
policy. Even in cases where the low risk is recognized, building owners
are compelled to remove asbestos for liability reasons and because
of the strong emotional impact of the risk.
radon
-
Radon-222 (Rn-222) is produced as part of the radioactive decay series from
U-238 to Pb-206. It is the daughter product of radium-226, and
decays itself to polonium-218 (Po-218), with a half-life of 3.8 days.
Radon exposure increases the risk of lung cancer, and is therefore
of public-health concern. Because radon is a gas, it can be inhaled into
the pleura easily. Its short half life means there is a finite chance
that Rn-222 will decay while in the lungs; polonium is not a gas, but a
solid, and therefore may become imbedded in the lungs, where the decay
chain can continue. The ionizing radiation from these decays can
damage genetic materials in the cells of the lungs, which can lead to
cancer. In addition, when radon decays to polonium in the air outside
the lungs, the solid decay products tend to become attached to
particles in the air. These particles are only slowly removed after
inhalation: they will tend to spend 3-30 minutes in the lungs before
they can be removed by the cilia. The four decay products following
radon-222 in the U-238 decay series have short half lives (1 microsecond
to 27 minutes); the probability that these decay products will themselves
decay while in the lungs is thus relatively high. Several of these decays
are also of the type (alpha decay) that tends to cause the tissue damage that
can lead to cancer.
[ the U-238 decay series ]
-
Exposure to radon depends mainly on where you live. Since Rn-222
is a decay product of U-238, radon concentrations will depend on the
uranium concentration in rocks. Several types of rocks tend to
contain high concentrations of uranium: felsic igneous rocks such as
granites contain high levels of uranium, as do black shales (formed
in the chemically reducing environment of the ocean bottom), and
sediments rich in phosphates. Bedrock type thus tends to control
the potential for radon exposure.
-
Radon tends to get into buildings through their basements after its
production by decays in surrounding bedrock. Since it is a gas, it is
mobile, and can filter out of the rock and into buildings through cracks
in the rock and building foundations. Radon will tend to concentrate
in poorly ventilated basements. Mitigation of the radon hazard can thus
be accomplished by improving basement ventilation, a relatively
straightforward and inexpensive procedure.
-
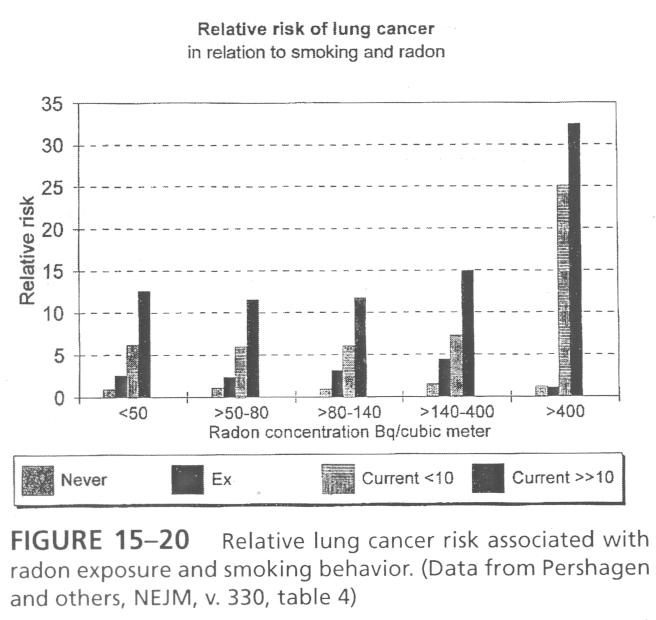
Epidemiological studies of excess deaths due to radon exposure highlight
an important aspect of this risk (one that is important for many
respiratory-disease risks): the risk of contracting lung cancer due
to radon exposure is strongly correlated with smoking behavior.
Non-smokers have a relatively low risk from radon exposure, while
smokers have a much higher risk, especially at high concentrations
of radon. The effect of smoking on lung cancer risk from radon exposure
is greater than additive, as can be seen in the chart attached.
[ relative risk of lung
cancer associated with radon exposure and smoking behavior ;
article on residential radon exposure for those interested in further information (you will need your Harvard ID and PIN) ]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}